Cherry-hued flecks dot the left half of his skull — grim mementos of the rocket-propelled grenade that walloped his armored vehicle in Baghdad last September. A bright scar bends like a stalk of rhubarb above his left ear, the result of six surgeries to treat the brain cancer doctors found while ministering to his shrapnel wounds; they fear the tumor was caused by depleted uranium that Pete, 28, handled as an Army mechanic.
And now, a plum-like bulge on his upper right jaw ripens before my eyes. This, oddly enough, is the one that really scares me: It’s the aftermath of a Marine’s clenched fist that hurled into Pete’s face just moments ago.
Only the bar gods know exactly how the skirmish began. But I’m guessing it went something like it did just the week before:
Lame invectives turn to blows. Soused onlookers hustle to their buddies’ defense. Only when a huge bouncer enters the fray do flying fists cease and desist — Marines head for the front exit, Army guys to the bar. As I search for ice to press against Pete’s busted cheek, the cops appear, looking downright bored by the redundancy of the mayhem.
Yes, sir, it’s another Friday night at R.J. Bentley’s Filling Station, a cozy bar in College Park, where wounded Iraq and Afghanistan veterans being treated at Walter Reed Army Medical Center come to fuel up on Coronas, honky-tonk dance and the “Rocky”-style pummelings I’ve seen on half a dozen visits this summer.
Venture here around dinnertime, and you’ll find University of Maryland professors eating fettuccine with their kids. But stay until the floors start getting sticky — say, around 11 p.m. — and it’s a different world altogether: a chance to brush up against college football hunks and thin girls in slinky tube tops, and also, perhaps, to witness some of the raw consequences of two faraway wars brought home.
Half a decade into the “war on terror,” America’s bars have become our barometers: instruments that measure the extent to which our veterans have been left to wrestle alone with substance abuse, anxiety disorders and other mental health problems after long tours in Iraq and Afghanistan.
The men and women who come back from the traumas of war “are often hyper-alert, quick to respond and susceptible to a loss of impulse control,” says clinical psychologist Jeffrey Jay of the Center for Post-Traumatic Stress Studies in Washington. “The brain is actually altered by these experiences — it’s part of a survival mechanism, and it’s very confusing for them.”
It’s similarly confusing for watering holes such as R.J. Bentley’s, where Pete likes to go because it’s the only bar around that occasionally plays the kind of country music he loves. “We’ve seen a massive rise in customers, thanks to Walter Reed,” one bouncer at Bentley’s told me. “But we’ve also seen a rise in fights.”
Police and news reports corroborate that fighting has been mounting in nightclubs, restaurants and bars near military bases nationwide: places such as McDonough’s Restaurant & Lounge near Fort Stewart, Ga.; O’Blarney’s Irish Pub south of Fort Lewis, Wash.; the entire “Strip” near Nellis Air Force Base in Las Vegas. Drunken driving and bar brawls so plagued the area around Fort Carson, Colo., that a National Guard unit was put on “lockdown status” after returning from Afghanistan in June. In the District, the Hawk ‘n’ Dove, a Capitol Hill bar, has banned Marines without female dates.
In Massachusetts, meanwhile, the Norfolk County district attorney’s office has begun an initiative called “Beyond the Yellow Ribbons” to prepare police and others to deal with struggling vets and the stigmas they face. District Attorney William R. Keating says he has received requests for the program’s training video from organizations in more than 20 states, because “the federal government simply isn’t providing enough guidance on how to deal with this.”
Perhaps that’s because the Bush administration’s $500 billion-plus “global struggle against violent extremism” has so far proved to be one of the most socially and economically quarantined conflicts in U.S. history. Whereas 12 percent of the population served in World War II and 4 percent in the Vietnam War, less than half of one percent of Americans are engaged in active duty in Iraq or Afghanistan. Translation: Only a sliver of my generation has been exposed to war’s dirty psychological laundry.
But with a growing number of troops returning home from multiple tours, more Americans like me — a 23-year-old occasional volunteer at Walter Reed and the girlfriend of a soldier serving in Iraq — are getting our first unsettling glimpse.
On a recent night at R.J. Bentley’s, I perched near a young man nursing a flask of whiskey who told me he’d been ordered to collect his best friend’s body parts from the crater of an improvised explosive device, and an older vet with darting eyes who said he’d tried to slit his wrists in Kuwait rather than return to Fallujah. And if you agree that trauma begets trauma, the evening’s trajectory won’t surprise you: Mix equal parts broken bodies and frayed minds, stir in college kids who couldn’t tell an IED from an iPod, add alcohol, and things are bound to get explosive.
I suspect these aren’t just the sort of routine bar fights that have typified military culture since George Washington’s troops sneaked their first swigs of moonshine. Strike Pete Yazgier, and you may slice your knuckles on his titanium skull. Toss an elbow at the man in the corner, and you could get a shin-kick from his $26,000 motorized foot, an emblem of the spectacular violence that new technologies are helping today’s troops survive.
The rough-and-tumble encounters jibe with national statistics on the effects of longer, repeated tours of duty. Soldiers who’ve deployed to Iraq more than once have a 50 percent higher rate of combat stress, according to one Army study, and soldiers with a higher rate of combat stress exhibit approximately a 10 percent increase in anger-management issues. Simple diagnoses such as “post-traumatic stress disorder” and “generalized anxiety disorder” collapse under the weight of it.
Consider Jonathan Schulze, an Iraq vet with two Purple Hearts who got drunk at a Minnesota bar in January, then went home and hanged himself from an electrical cord wrapped around a beam in his basement. The tragedy unfolded only after the Marine machine-gunner returned from Ramadi with deep psychological wounds, threw a 200-pound potted tree through a window during a brawl, and beseeched the local Veterans Affairs Department for help, only to be told that his suicidal confessions put him 26th on the waiting list for assistance. (According to a recent Pentagon report, suicide rates are 35 percent higher for Iraq veterans than for the general population.)
Then there are cases like that of Spec. Richard Davis, who survived “shock and awe” in Baghdad only to be stabbed to death by his fellow soldiers in 2003 after celebrating his homecoming at a Hooters restaurant and a topless bar near Fort Benning, Ga.
Institutional ignorance isn’t the problem. In January, the Pentagon released a survey cautioning that the rate of binge drinking in the Army skyrocketed 30 percent between 2002 and 2005, hurting combat readiness. Even so, the best response the Defense Department could muster was a Web-based campaign called “That Guy,” which goofily implores soldiers to “Turn your speakers on, dude!” so that they can hear cartoon-animated warnings about how guzzling beer might hurt their sex lives by causing them to puke in their date’s purse.
Perhaps the $2 million this cost would have been better spent on comprehensive treatment programs for servicemen and women of the sort that are sorely lacking at Walter Reed, where the renowned PTSD program accepts a paltry average of 65 patients a year and a typical mental health regimen involves, according to a report in The Washington Post, random screenings of movies such as “The Devil Wears Prada” and a dearth of one-on-one therapy with trained clinicians.
In my own small way, I’ve seen the price of this negligent government policy, coupled with the military stigma against seeking help for psychological distress. I’ve sat outside the hospital with Pete’s friends as they drank heavily, talked about friends’ corpses, compared R.I.P. tattoos and fed their psych meds to the squirrels to pass the slow-drip nights. I’ve held the forehead of my courageous boyfriend, Robert, as he shivered on the cold tile floor of our hotel room, vomiting Scotch, on our last vacation in January, before his most recent deployment. We laughed at his New Year’s resolution — “Don’t get blown up” — but all the while my brain screamed, “This can’t be normal!” because, well, my heart knew it wasn’t, and because I sensed the deeper pain his jokes masked.
“You don’t get the option to not be scarred by war,” he recently wrote me from Iraq. “You don’t get to shed your uniform and go home like nothing’s different. You forever carry the seeds of violence inside.”
Those seeds are sprouting like strangle-weed as the rest of America bustles along, debating the fates of Posh Spice and Harry Potter, as if war were just a pixilated thing that happens to far-away Muggles. Some of these weeds can be uprooted: More than 45,000 vets overcame the stigma of PTSD to seek medical help in the first quarter of 2007, and national legislation such as the Wounded Warriors Act promises to funnel more resources toward vets’ mental health, if it ever escapes congressional molasses.
But much of the current wars’ noxious overgrowth is proving ineradicable, coiling stealthily around our bars, jails, businesses and private lives.
One damning manifestation is traumatic brain injury (TBI), the unforeseen consequence of modern military technologies and equipment such as Kevlar helmets. Sixty percent of all injured vets entering Walter Reed suffer from TBI as a primary or secondary injury, according to the Defense and Veterans Brain Injury Center.
Three of the four most notorious troublemakers I’ve gotten to know at R.J. Bentley’s are victims of TBI — a silent disability that receives little of the public sympathy afforded the war’s more visible amputees. And there’s no snazzy Web site or government program that will undo cranial nerve damage or recover a personality that has fallen off the tip of its own tongue — slow to remember, quick to violent outbursts, unrecognizable to loved ones.
On a recent night, I loaded up the car with TBI-afflicted friends, including Pete (who, for the record, is funny and smart and kind), and drove to a happy-go-lucky bar in Adams Morgan in the District, where the drinks come with cheerful pink umbrellas.
Approaching the bar, we saw a blond guy with a cast on his wrist. “Hey, you were in Iraq, too?” asked Pete’s friend Zach, tapping the cast. The kid looked befuddled. “No — I just fell at the pool.”
The exchange was a perfect reflection of how the true costs of war have been outsourced to a very few Americans, and a great many Iraqis. But it also reminded me that full-scale containment of the wreckage is impossible — that, as Nigerian novelist Chinua Achebe wrote of imperial ventures in years past, “things fall apart.”
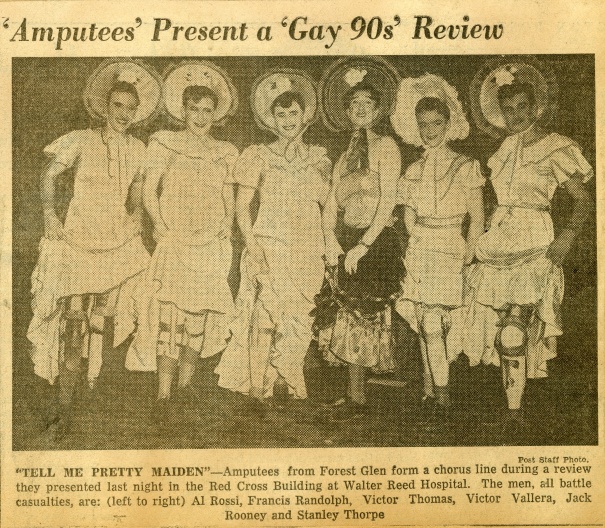
 For Veteran’s Day, I wrote a brief story for the Dart Society Reports on “sex and the wounded soldier.” It’s about a lot of overlapping themes — my friendship with a wounded soldier (now dead) who worried a lot about war’s impact on his intimate life; an amputee dance troupe from World War II, called “The Amputettes”; the U.S. military’s long-standing awkwardness about matters of sex, heart, and family. It all seems a bit more timely with the Petraeus love triangle (quadrangle? pentagon? hexagon?).
For Veteran’s Day, I wrote a brief story for the Dart Society Reports on “sex and the wounded soldier.” It’s about a lot of overlapping themes — my friendship with a wounded soldier (now dead) who worried a lot about war’s impact on his intimate life; an amputee dance troupe from World War II, called “The Amputettes”; the U.S. military’s long-standing awkwardness about matters of sex, heart, and family. It all seems a bit more timely with the Petraeus love triangle (quadrangle? pentagon? hexagon?).